here::i_am("Model_implementation_validation/quarto/valid_amox_carlier_2013.qmd")# Functions used for simulation-----# export functions contained in the "functions" folderlist_of_function_path =list.files(path = here::here("Model_implementation_validation/R_functions/"),pattern =".*\\.R$",full.names =TRUE ) purrr::walk(.x=list_of_function_path,.f=source)
Typical clearance (for a patient with creatinin clearance of 102 mL/min)
L/h
10.0
Q
Intercompartmental clearance
L/h
15.6
Vcpop
Typical central volume of distribution (for a patient with creatinin clearance of 102 mL/min)
L
13.7
Vp
Peripheral volume of distribution
L
13.7
cv_iiv_CL
Coefficient of variation of the inter individual variability on clearance (%)
unitless
39.9
cv_iiv_Vc
Coefficient of variation of the inter individual variability on central volume of distribution (%)
unitless
38.7
ruv
Coefficient of variation of the residual variability
unitless
22.0
3.2 Inter-individual variability and covariate effects
Covariate effect : \[
TVCL_{i} = CLpop*\frac{CLCR_{i}}{102}*e^{\eta_{i}}
\] With : \(TVCL_{i}\) : Amoxicillin clearance for individual i \(CLpop\) : Typical amoxicillin clearance (L/h) \(CLCR_{i}\) : 24h urinary creatinin clearance (mL/min) for individual i \(\eta_{i}\) : Normal variable with mean 0 and variance \(\omega^2_{CL}\) \(102\) : population’s median urinary creatinine clearance in mL/min
4 Validation of the mrgsolve implementation of the amoxicillin model
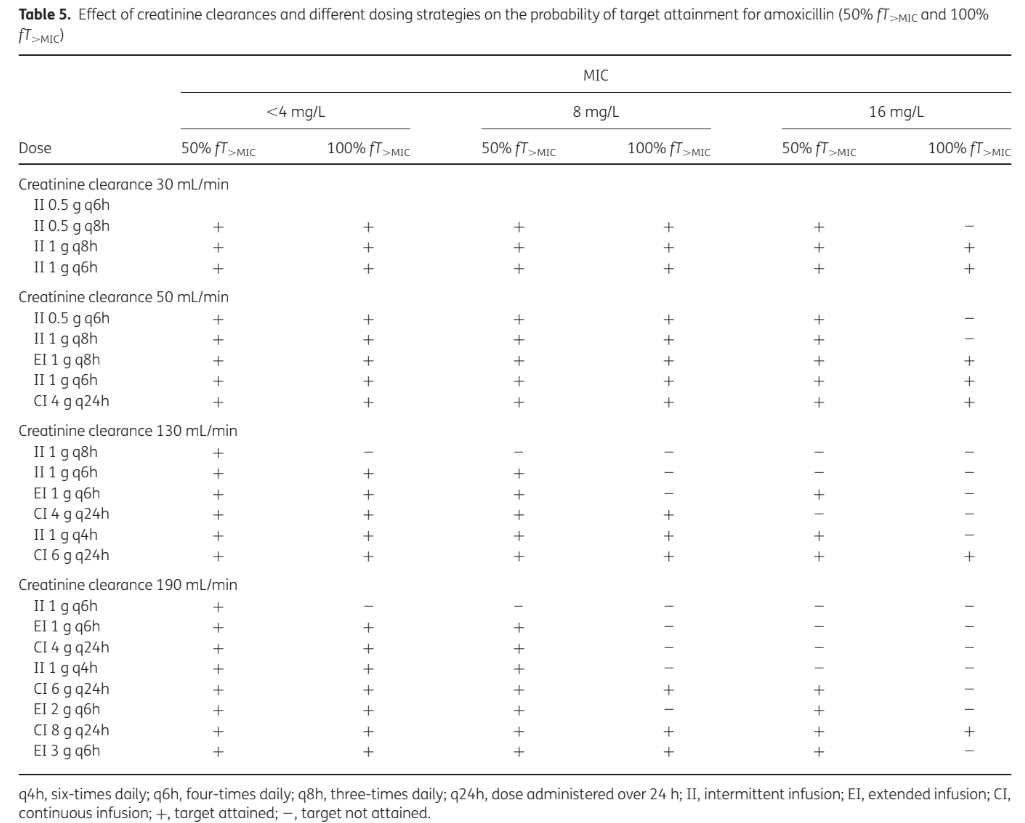
To validate that our implementation of the model is correct we will attempt to reproduce figure 2 and table 5 of the original article.
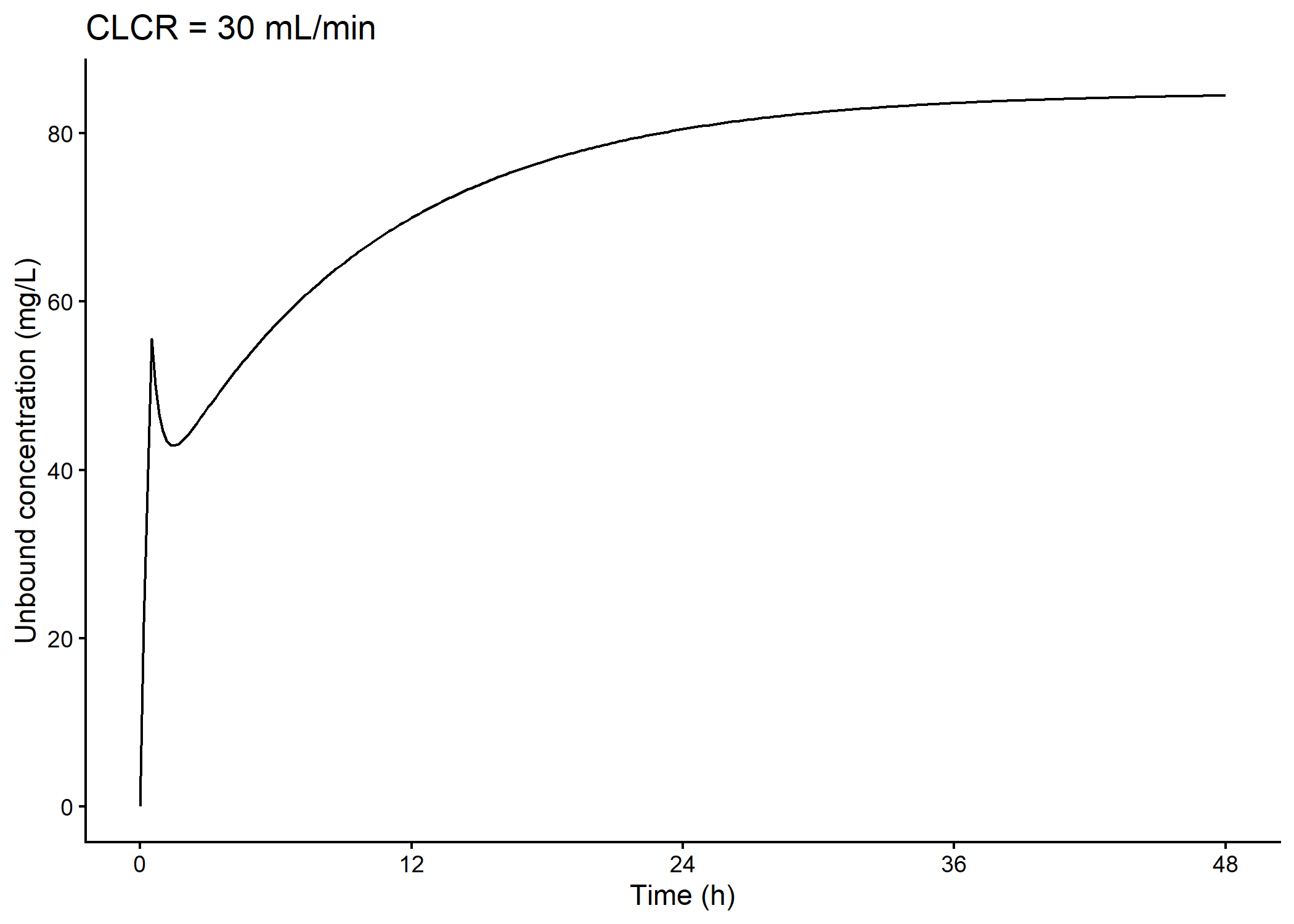
4.1 Preliminary testing
First we check that simulations for a single dosing regimen and creatinine clearance value make sense.
This table indicate wether the target is attained for a typical patient receiving amoxicillin, for various dosing regimen and various creatinin clearances.
Aside from one dosing regimen (ci 4g q24h for a CLCR of 190 mL/minutes), disagreements between table 5 and our simulations are underestimations of the fT>MIC.
A lot of these disagreements imply differences between the fT>MIC that we simulated and table 5 close to 10%.
The dosing regimens for wich there is more difference are :
for a creatinin clearance of 130 mL/min and a MIC of 4 mg/L, “ii 1g q6h” ;
for a creatinin clearance of 130 mL/min and a MIC of 16 mg/L, “ei1g q6h” ;
for a creatinin clearance of 190 mL/min and a MIC of 4 mg/L, “ei 1g q6h” ;
for a creatinin clearance of 190 mL/min and a MIC of 8 mg/L, “ci 4g q24h” and “ei 3g q6h” ;
for a creatinin clearance of 190 mL/min and a MIC of 16 mg/L, “ci 6g q24h”.
We seemed to underestimate fT>MIC for higher creatinin clearances more than lower ones.
No kind of dosing regimen (continuous, extended or intermittent infusion) looked more susceptible to disagreements between our simulations and table 5.
For continuous infusions, we obtained fT>MIC equal to 0% or close or equal to 100%. However, in table 5, for a CLCR of 190 mg/L and a MIC of 16 mg/L, we notice that for he dosing regimen “Ci 6g q24h”, the target of fT > MIC >= 50% is atteined but not a fT > MIC of 100%. This may indicate that the article’s author didn’t perform calculate fT > MIC at steady state only. Instead, they may have included the loading dose in the time interval used to calculate fT > MIC.
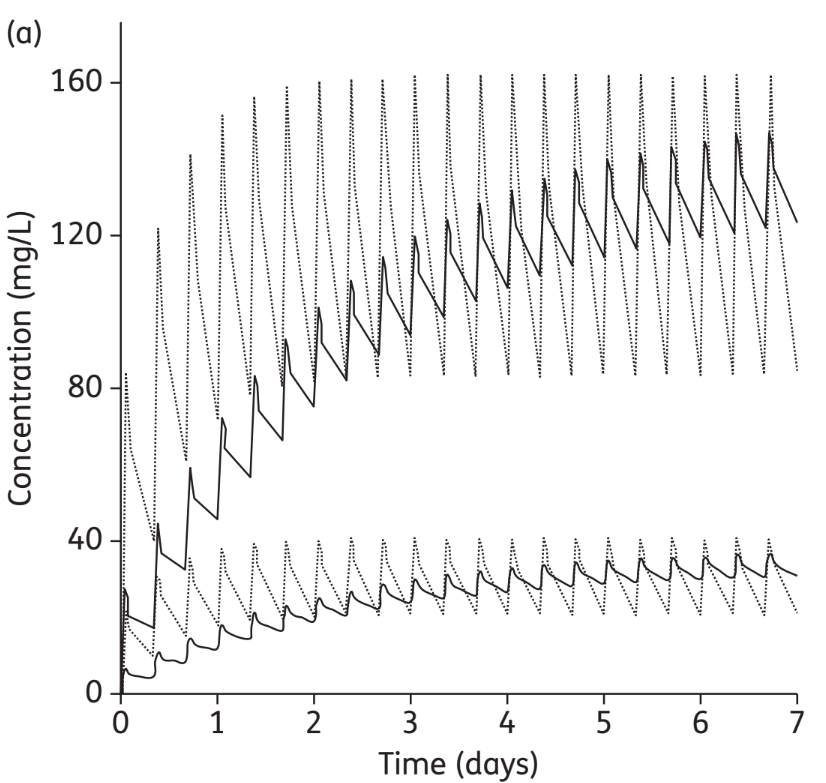
We noticed that the authors simulated 7 days of treatment to create figure 2. We hypothesized that they also simulated 7 days of treatment and calculated fT > MIC on all the simulation duration in order to create table 5. We then calculated fT > MIC on seven days of treatment (results not shown here). This yielded results similar to the one obtained on 24 hours at steady state : we observed disagreements for the same dosing regimens, MIC and CLCR and fT > MIC equals or slightly inferiors. In particular, for a CLCR of 190 mg/L and a MIC of 16 mg/L, we still obtained a fT > MIC equal to 0%. We didn’t confirm our hypothesis.
We also calculated fT > MIC on the first 24 hours of treatment. However, the fT>MIC were underestimated compared to the results of the article and there were a lot more disagreements between our simulations and table 5. For a CLCR of 190 mg/L and a MIC of 16 mg/L, fT > MIC was only equal to 9%.
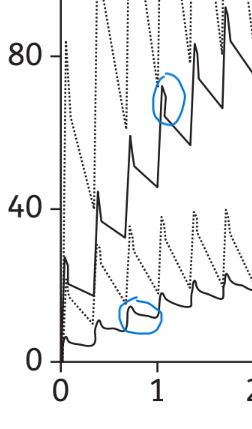
4.3 Figure 2
While it would seem that Figure 2 could also be used for validation of our model implementation, careful consideration of the plot makes us suspect that technical errors happened while preparing the figure. Therefore, no attempt at reproducing the figure will be made.
4.4 Conclusion
We think our mrgsolve model is an adequate representation of the published model since :
The equations and parameters values of our mrgsolve model are identical to the reported ones
Most fT>MIC were accurately reproduced
The slight discrepencies could be due to different simulation settings (e.g. different time points) and/or missing correlations between variability parameters which were not reported.
Carlier, Mieke, Michaël Noë, Jan J De Waele, Veronique Stove, Alain G Verstraete, Jeffrey Lipman, and Jason A Roberts. 2013. “Population Pharmacokinetics and Dosing Simulations of Amoxicillin/Clavulanic Acid in Critically Ill Patients.”J. Antimicrob. Chemother. 68 (11): 2600–2608.